|
抗磷脂質症候群與生殖困境
抗磷脂質症候群(Antiphospholipid syndrome,APS)容易造成血栓影響動靜脈循環,最常被影響的靜脈是下肢深層靜脈,動脈則是腦血管[1],然而,全身各種組織及器官的血管網都有可能被影響,在小部分病人身上會同時造成多重器官衰竭,因具有很高的死亡率,故稱為災難性抗磷脂症候群(catastrophic antiphospholipid syndrome)。[2]特別的是,在形成血栓的位置並沒有找到任何發炎的跡象。[3]抗磷脂質症候群的另一項臨床特點是影響懷孕,會造成找不出原因的流產、早產、子癲前症。
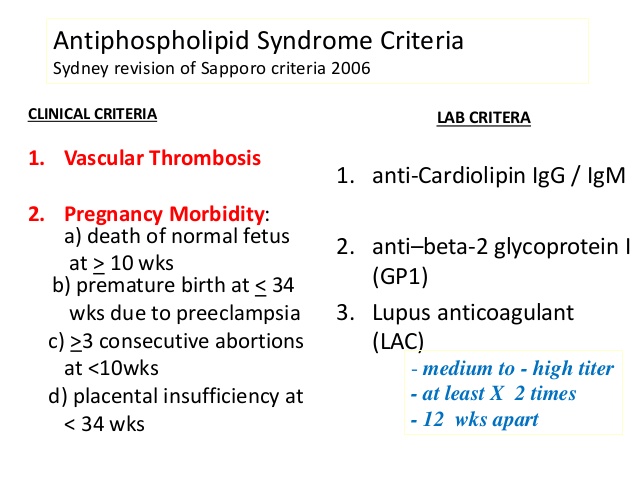
依據2006年編定的抗磷脂質症候群診斷標準,強調要確診APS必須同時符合臨床及實驗室診斷標準中的一項,該標準如下:
一般所說的Antiphospholipid antibodies(aPL)泛指上面所說的三項,有研究指出Lupus anticoagulant(LA)比起anti–β2-glycoprotein I(anti–β2GP I)、anticardiolipin antibodies(aCL)是一項更容易形成血栓的危險因子,如果在懷孕12週後檢出LA很可能會出現不良的併發症。[4-6]
有將近1%的女性受重複性流產所苦,這當中又有10-15%帶有抗磷脂質症候群[7],LA可預測這些女性後續是否會發生血栓,若LA陽性每年發生深層靜脈栓塞的機率為1.46%,發生中風的機率為0.32%[8]。
雖然LA較能預測未來發生血栓的機會,但抗磷脂質症候群的病理機轉與anti–β2GP I比較有關,這些自體抗體會與B cell上的β2-glycoprotein I分子結合,藉此賦予LA活性增加後續發生血栓的風險[9]。許多研究發現抗磷脂質症候群與氧化壓力(oxidative stress)有很大的關係,學者發現APS患者身上的Paraoxonase (一種抗氧化酶)明顯減少[10-11],而8-epi-prostaglandin F2α(一種過氧化物)則增加[12],氧化壓力會改變β2-glycoprotein I分子的結構與功能,如下圖所示,進而誘發免疫免疫並促使血栓形成。

參考資料:
[1] Cervera R, Piette JC, Font J, et al. Antiphospholipid syndrome: clinical and immunologic manifestations and patterns of disease expression in a cohort of 1,000 patients. Arthritis Rheum 2002;46:1019-27.
[2] Cervera R, Bucciarelli S, Plasin MA, et al. Catastrophic antiphospholipid
Syndrome (CAPS): descriptive analysis of a series of 280 patients from the “CAPS
Registry.” J Autoimmun 2009;32:240-5.
[3] Miyakis S, Lockshin MD, Atsumi T, et al. International consensus statement on
an update of the classification criteria for definite antiphospholipid syndrome (APS). J Thromb Haemost 2006;4:295-306.
[4] Galli M, Luciani D, Bertolini G, Barbui T. Lupus anticoagulants are stronger risk
factors for thrombosis than anticardiolipin antibodies in the antiphospholipid
syndrome: a systematic review of the literature. Blood 2003;101:1827-32.
[5] Urbanus RT, Siegerink B, Roest M,Rosendaal FR, de Groot PG, Algra A.
Antiphospholipid antibodies and risk of myocardial infarction and ischaemic stroke in young women in the RATIO study: a case-control study. Lancet Neurol 2009;8:998-1005.
[6] Lockshin MD, Kim M, Laskin CA, et al. Prediction of adverse pregnancy outcome by the presence of lupus anticoagulant, but not anticardiolipin antibody, in patients with antiphospholipid antibodies. Arthritis Rheum 2012;64:2311-8.
[7] Ruiz-Irastorza G, Crowther M, Branch W, Khamashta MA. Antiphospholipid syndrome. Lancet 2010;376:1498-509.
[8]Gris JC, Bouvier S, Molinari N, et al. Comparative incidence of a first thrombotic event in purely obstetric antiphospholipid syndrome with pregnancy loss: the NOH-APS observational study. Blood 2012;119:2624-32.
[9] de Laat B, Derksen RH, Urbanus RT,de Groot PG. IgG antibodies that recognize epitope Gly40-Arg43 in domain I of beta 2-glycoprotein I cause LAC, and their presence correlates strongly with thrombosis. Blood 2005;105:1540-5.
[10] Delgado Alves J, Ames PR, Donohue S, et al. Antibodies to high-density lipoprotein and beta2-glycoprotein I are inversely correlated with paraoxonase activity in systemic lupus erythematosus and primary antiphospholipid syndrome. Arthritis Rheum 2002;46:2686-94.
[11] Charakida M, Besler C, Batuca JR, et al. Vascular abnormalities, paraoxonase
activity, and dysfunctional HDL in primary antiphospholipid syndrome. JAMA 2009;302:1210-7.
[12] Ames PR, Nourooz-Zadeh J, Tommasino C, Alves J, Brancaccio V, Anggard EE.
Oxidative stress in primary antiphospholipid syndrome. Thromb Haemost 1998; 79:447-9.
|











